Most who take levothyroxine (LT4) do so once a day.
Many who take liothyronine (LT3) do so more than once a day. (Though some do prefer once a day dosing.)
Many who take desiccated thyroid do so more than once a day.
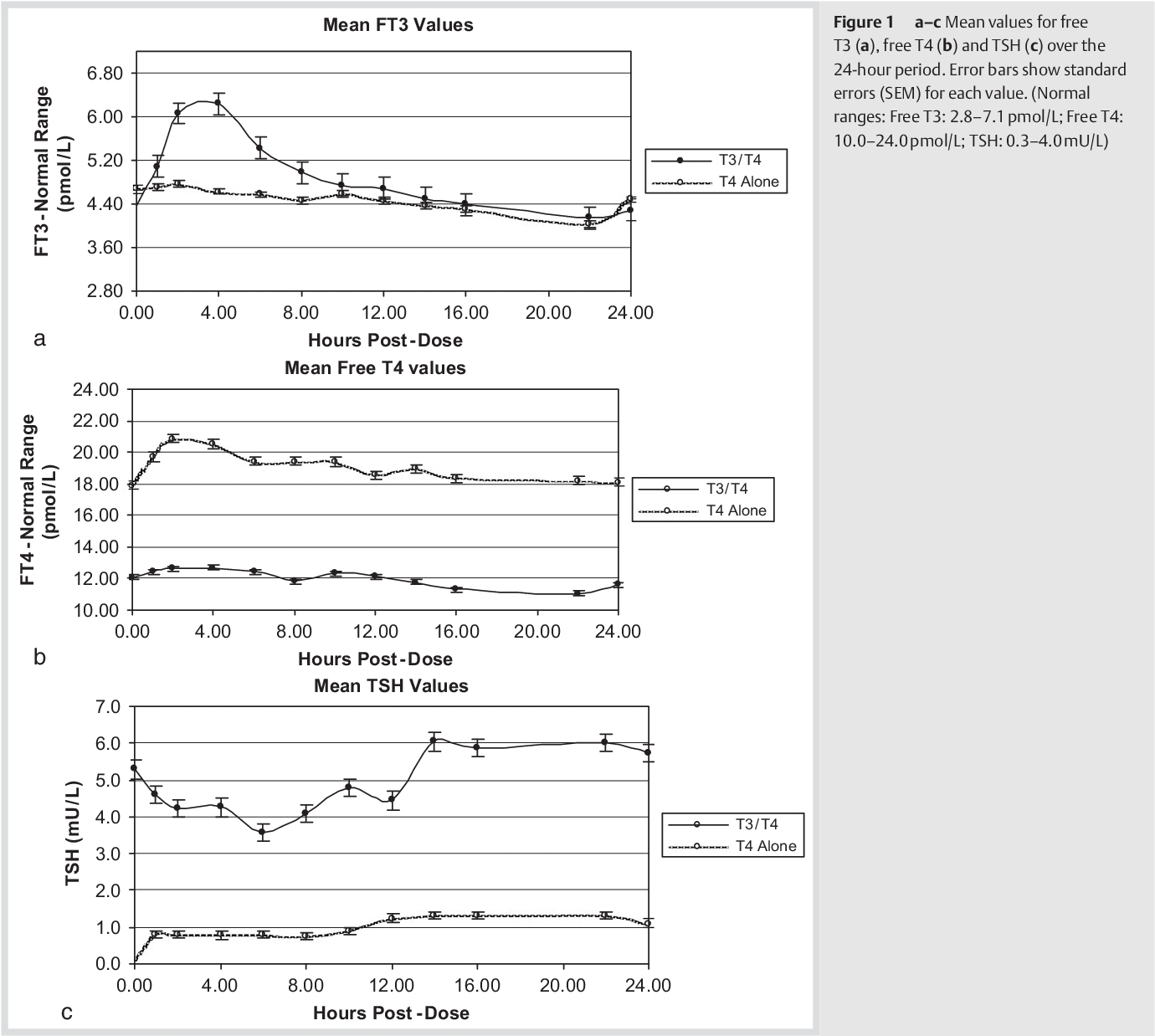
From taking LT4 or LT3 to peak blood levels typically takes two to four hours. (Assuming taking on an empty stomach.)
The sharp peak of FT4 and/or FT3 after dosing means that it is hard to draw blood at the precise peak. When sequential blood draws have been performed in research, even a few minutes could make a difference. If only doing a single blood draw, the timing of the peak is necessarily guesswork.
From the sharp peak, both FT4 and FT3 fall away, faster at first, slowing later. The time immediately before the next dose is often called the trough. (FT4 drops more slowly than FT3.)
(The sharpness of the peak is not so clear for FT4. It would be very much more obvious if the origin of the graph were shifted to approximately the trough level. But that would be inappropriate.)
At any point from the peak - for several hours - there is an appreciable rate of change. Therefore timing would be expected to affect the result.
Because the rate of change in the trough is low, precise timing is not so important.
For these reasons, it appears that blood draws should be done consistently in the trough. That will achieve maximum comparability of results from one test to the next.
It might be suggested that all results could be interpreted, regardless when the blood was drawn, by applying various "corrections". This has some appeal but we are all different. If we knew our own profiles, we might be able to make some educated guesses. But we don't. So any attempt to correct is based far too much on guesses. Also, it would be very unusual for someone to be asked when they took their last dose.
An ideal might be continuous monitoring (as is now being achieved for glucose in diabetes). Next, something like hourly measurements. But neither of these is remotely feasible outside research.
Increased fT4 concentrations in patients using levothyroxine without complete suppression of TSH.
In conclusion, the observed fT4 concentrations above the ULN together with not (completely) suppressed TSH were not caused by incorrect reference intervals or analytical problems but mainly related to L-T4 use. Most likely, a combination of timing of blood withdrawal and the timing of L-T4 intake causes this phenomenon.
https://europepmc.org/article/MED/36762702

As so often, Tania at Thyroid Patients Canada has already done an excellent article:
Free T3 peaks and valleys in T3 and NDT therapy
November 25, 2019
https://thyroidpatients.ca/2019/11/25/free-t3-peaks-and-valleys-in-t3-and-ndt-therapy/
Previous HealthUnlocked posts on this subject which have much more detail:
Suggested Thyroid Hormone Test Timing Protocols
radd
https://healthunlocked.com/thyroiduk/posts/149327184/suggested-thyroid-hormone-test-timing-protocols
Timing and reasons for Thyroid blood tests
This UK lab offers an explanation of timing issues:The Impact of Natural 24-Hour Fluctuations on Blood Test Results
https://thriva.co/hub/community-health-insights/diurnal-result-variation
SlowDragon
https://healthunlocked.com/thyroiduk/posts/150755641/timing-and-reasons-for-thyroid-blood-tests
The following quotes are somewhat old and are far from ideal. However, they do have some interest:
In monitoring patients with hypothyroidism on L-thyroxine replacement, blood for assessment of serum free T4 should be collected before dosing because the level will be transiently increased by up to 20% after L-thyroxine administration (72.). In one small study of athyreotic patients, serum total T4 levels increased above baseline by 1 hour and peaked at 2.5 hours, while serum free T4 levels peaked at 3.5 hours and remained higher than baseline for 9 hours (72.).
Clinical Practice Guidelines for Hypothyroidism in Adults: Cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association
ATA/AACE GUIDELINES| VOLUME 18, ISSUE 6, P988-1028, NOVEMBER 2012
https://www.endocrinepractice.org/article/S1530-891X(20)43030-7/fulltext
DOI: https://doi.org/10.4158/EP12280.GL
Although not recommended, if used, the following common sense recommendations to monitoring might apply. LT3-only therapy should be monitored with measurements of fasting serum TSH levels before the administration of the dose, aiming to target serum TSH within the lower tertile of the reference range, if aiming for TSH values seen in a normal population (54). Although data to support this approach are not available, it would seem reasonable to measure serum T3 levels in the morning (trough) and 2 hours after the administration of the dose (peak), aiming to maintain the values within the reference range; serum FT4 assessment is of no value in this scenario.
Guidelines for the Treatment of Hypothyroidism: Prepared by the American Thyroid Association Task Force on Thyroid Hormone Replacement
https://www.liebertpub.com/doi/full/10.1089/thy.2014.0028
Blood Levels vs Cell Levels
The true meaning of blood levels is frequently ignored. Blood is very much the carrier of thyroid hormones. Their actual effects take place within cells. The blood level matters because it carries the thyroid hormones (because conversion adds complexity, I'll only consider T3) and makes them available to our cells.
As we approach our next peak T3 level, we must consider that our cells are just undergoing a period of low T3. Therefore they are ready to take in more T3 than would be the case if the T3 level were very even.
Instead of the cells getting their T3 more or less randomly, many
of them receive their T3 within a short period of time. More shortly
after a dose, and less shortly before the next dose.
It does not mean that the total amount of T3 taken in by cells in a full day is higher.
This contrasts with hyperthyroidism, where the T3 level is high all day, every day, as happens in Graves' Disease. The cells get too much T3. And the person suffers.
When taking T3, the T3 level will be relatively high shortly after each dose. If we split the dose, that makes the variations between the blood peaks and troughs smaller. Which seems like a good idea and many who take T3 prefer that.
But maybe our bodies are actually better able to handle a single larger trough to peak difference? I suggest that if our bodies react to an excess of T3, they might excrete some of the excess. This would tend to limit the height of the peak and also limit the amount of T3 available for use. This could mean that, for a given total daily intakes of T3, taking it in a single dose allows our bodies to handle it better than when split across multiple doses?
Short of some sort of continuous dosing being available, we need to use the approach which works best for us.
Other Factors
Fasting
It is usual in the UK to say that fasting is not necessary for thyroid blood tests.
However, fasting is required for some blood tests.
You could end up sometimes having thyroid blood tests done when fasting, sometimes not.
Even if the difference is modest, always fasting avoids even that test to test variation. And when doctors sometimes make decisions on small differences, this can be very important.
It is also not uncommon to find out afterwards that tests have been run which are more affected by fasting that thyroid tests.
The simple approach of always fasting seems the best to achieve comparable results over time.
More recently, it has been shown that TSH is significantly affected by calorie intake. Which makes fasting appear even more the right choice.
Effects of calorie intake and sampling time on thyroid stimulating hormone concentration
Background
This study aimed to investigate the effects of blood sampling after calorie intake on thyroid stimulating hormone (TSH) level, compared with blood sampling in fasting state.
Conclusion
In summary, the TSH level was reduced significantly after food intake, compared with that at fasting state in the morning. If the reference range of TSH used in the laboratory was from fasting blood samples, it would be better to evaluate the TSH level in fasting blood obtained in the morning compared with random or postprandial samples.
https://bmcendocrdisord.biomedcentral.com/articles/10.1186/s12902-022-01005-7
Effect of Pre- and Postprandial Plasma Glucose Levels on Thyroid Hormones: A Cross-Sectional Study
Abstract
Background
There is not much data regarding the effect of plasma glucose on thyroid hormones. Currently, there is no consensus regarding the timing of blood sample collection for thyroid hormones. Evaluation of the correlation between plasma glucose and thyroid hormones may enhance pathophysiological understanding of postprandial thyroid stimulating hormone (TSH) decline.
Objectives
To study the effect of pre-and postprandial plasma glucose levels on thyroid hormones.
Methodology
A cross-sectional study was done among participants aged 18 years and above after obtaining informed consent. Venous blood samples for fasting and postprandial plasma glucose, fasting, and postprandial thyroid profile ((FT3), (FT4), and TSH) were collected. The association was studied using the t-test and chi-square test between groups, while correlation using Pearson’s correlation coefficient. A p-value of <0.05 was considered statistically significant.
Results
Among the 197 participants, 126 (64%) were female and 71 (36%) were male. The mean (± S.D.) of age was 43.74 (± 12.62) years. Mean (± S.D.) postprandial TSH (4.31 μU/ml (± 7.79)) and free T3 (285.52 pg/dl (± 32.46)) were less than the fasting values (4.99 μU/ml (± 7.78)) and (295.84 pg/dl (± 32.56)). The mean (± S.D.) of both fasting and postprandial TSH and free T4 were less in the high plasma glucose group compared to the normal plasma glucose group (fasting state p-values 0.005, <0.0001 & postprandial state p-values 0.016, <0.0001). The correlation between fasting plasma glucose and fasting TSH values (Pearson correlation; r=-0.18; p-value 0.232) was observed across all the plasma glucose ranges.
Conclusion
There is a significant postprandial decline in TSH levels than the fasting TSH, indicating that there is a plasma glucose-mediated reduction in TSH values.
Hydration/dehydration
In order to obtain a good sample, adequate hydration is necessary.
Having a drink half an hour before a blood draw is not sufficient. Don't drink large or excessive quantities but pay extra attention to hydration for the full day before your blood draw.
Skin
Do not apply any treatments whatsoever (sun lotions, moisteners, bronzers, or anything else) to the area of skin from which blood will be drawn.
Blood Flow
Modest movement - such as walking - can help to ensure that blood is easier to obtain.
Vitamins and Supplements
Some vitamins and supplements can affect blood draws and assays. There is such a large number of products, it is impossible to summarise in a few words. However, there is a specific blog to read if you take any supplements contain biotin is large amounts.
helvella - Biotin supplementation and testing
A short article about how and why biotin can affect blood tests. Includes information about how to avoid any problems.
Last updated 04/08/2024.
https://helvella.blogspot.com/p/helvella-biotin-supplementation-and.html
If you wish to link to this page on HealthUnlocked, copy the entire dark red text below and paste into a post or reply.
[i][b]helvella - Scheduling Blood Draws [/b]
Factors to consider when choosing time for blood draws. Includes links to several documents/webpages and previous HealthUnlocked posts.
Last updated 14/10/2025[i]
Link to blog:
https://helvella.blogspot.com/p/helvella-scheduling-blood-draws.html
If you find anything incorrect, misleading, typos, links
that don’t work, etc., please let me know. Go to my profile and use the contact details there: